In the past twenty years, the term “design thinking” has entered mainstream and business lexicon to describe a methodology for generating innovative solutions. The renowned design firm, IDEO, popularized and marketed the idea as a cross-disciplinary tool to help individuals and organizations identify challenges and develop novel solutions. It has been used in a variety of fields like healthcare, business, and education. Design thinking principles focus on the end-user, whether it is the patient, the client, or the student. It is a process that requires research and collaboration, openness and curiosity, and the willingness to experiment.
A special characteristic of design thinking that makes it a valuable tool is its emphasis on prototyping solutions to test them before bringing an actual product or concept to the real world. By testing prototypes, designers can understand the strengths and weaknesses of a solution, and then iterate on the solution by making small changes to the prototype to refine the idea.
Design thinking has helped transform healthcare organizations like Kaiser Permanente and the Mayo Clinic so that they can better serve their patients. More recently, it has seeped into healthcare education, as Jefferson Medical College in Philadelphia now offers a formal design program for medical students. Conferences like TEDMED, Stanford MedX, and even South by Southwest have made the marriage of design and healthcare more popular. The methodology is helping us reimagine the future of medicine.
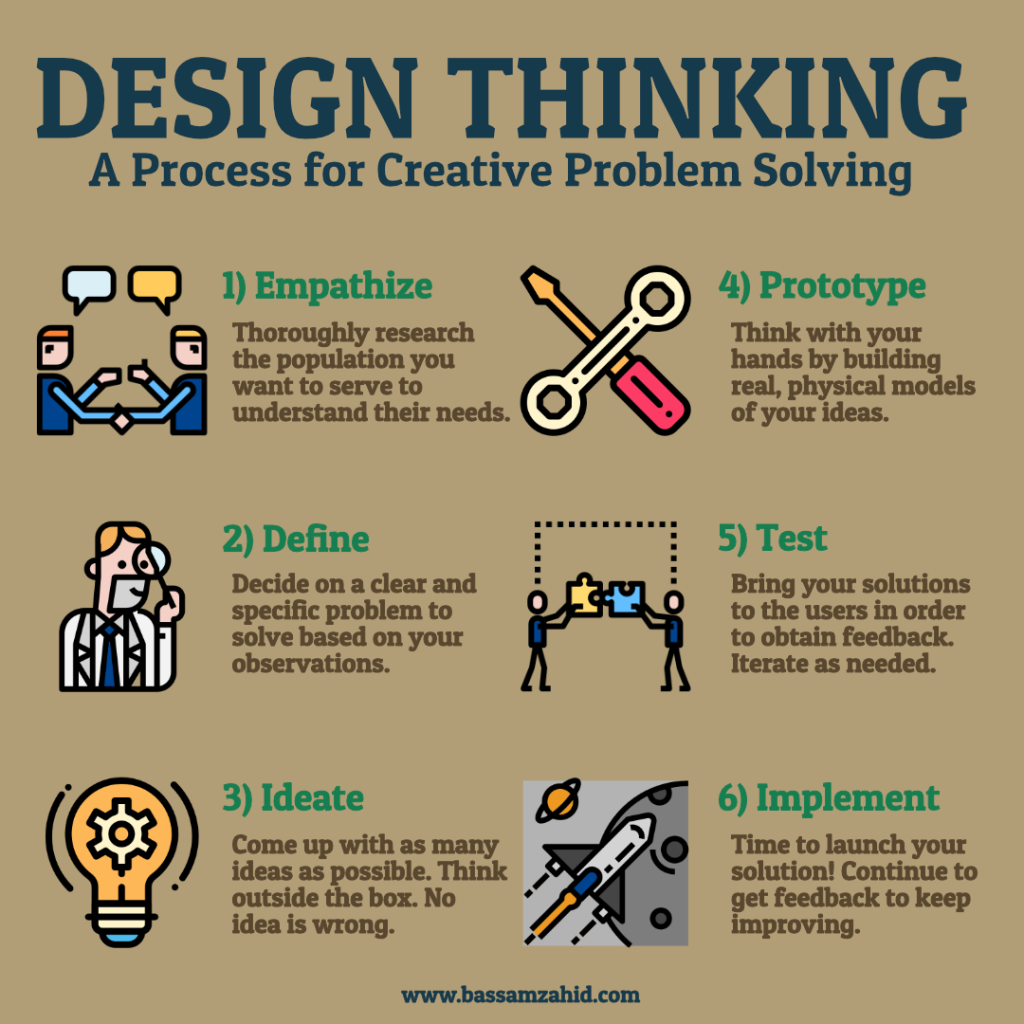
Design thinking consists of six steps: empathize, define, ideate, prototype, test, and implement. Let’s break them down.
Empathize
The foundation of design thinking is human-centered innovation. This marked a break from the traditional concepts of design and engineering, which had emphasized only functionality. Now, designers are also concerned about how the final solution resonates with the client emotionally. Do we understand what the client wants? Can we meet them where they are at? How do they feel about it?
Accomplishing this task requires in-depth research on the habits and lifestyle of the client. Let’s say we are trying to understand the needs of patients as they navigate the emergency department. This would require observing them in the waiting room, watching them fill out forms and interact with the nurses, and following them all the way to discharge. We would have to understand the emergency department from the perspective of the patient. Does it make them feel safe? Are they comfortable? Do they understand what is going on? Is the experience as pleasant as it could be? We would also have to ask anyone involved, from the receptionist to the tech to the physician, where the system was efficient and effective and where the points of frustration slowed the process down.
Most importantly, beyond their experience in the emergency room, it is essential that we gather information about the life of the patient outside of the ER. What brought them there? If it was not an emergent condition, why did they come? What are their barriers to healthcare that might increase the chances that they return? How can we minimize it?
Define
Synthesizing the experiences of the staff, the doctors, the nurses, and the patients gives us a better understanding of how to meet the client’s needs. We can identify specific goals and problems to focus our attention. Perhaps the nurses and doctors aren’t communicating effectively and the patients are being asked the same questions repeatedly. Or maybe the workflow on the electronic health record lacks efficiency and so physicians are getting bogged down by data entry. Having a well-defined vision makes it easier to develop steps towards an effective solution.
Sometimes, a problem expressed by the client is not the actual issue. A patient complaining of long ER wait times might not be due to convoluted intake forms or an inexperienced receptionist, but could be due to the fact that the rooms are not being cleaned fast enough because the cleaning supply closet is not easily accessible to hospital staff. By gathering enough information about the patients’ journey through the ER, we can have a clearer picture of where the solution may lie.
Ideate
Now it is time to brainstorm. The process of ideation requires divergent and convergent thinking. In the former, we are trying to trying to create as many choices as possible. This is where the innovation happens. In the latter, we are trying to make choices based on practicality. This is where reality happens.
We want to think of as many solutions as possible, while keeping in mind that the solution must be human-centered. Every idea should be considered. There is no such thing as a bad idea. The more ideas, the better. Think outside of constraints as much as possible. Gather diverse perspectives. Take a cue from improv comedy and use the words “Yes and…” to build on each other’s ideas. Most importantly, don’t judge. This is divergent thinking.
Of course, life is not a vacuum and the solution must ultimately be feasible, replicable, and cost efficient. So towards the end of the process, it is important to make decisions on which ideas to pursue. Which ideas are scalable? Which ones deliver the most bang for the buck? Which ones are realistic? This is convergent thinking.
Prototype

What makes design thinking so powerful is that it is easy to pursue multiple solutions at once. By prototyping ideas, multiple teams can get a sense of which solutions might work. The founder of IDEO, David Kelley, called prototyping “thinking with your hands.” There does not have to be a single perfect idea. So build your vision. Break out the craft supplies. Construct a model of the ER or the patient’s room using cardboard or popsicle sticks or even legos. Create diagrams and drawings. Conduct role plays.
The prototype should not be a refined solution, but a rough concept, limited in scope. Time, effort, and cost should only be enough to generate some understanding on whether or not the idea works and if it should be pursued further. As the process continues, the number of prototypes will decrease, while the complexity and specificity of each model increases.
Test and Iterate
Very rarely do we get a solution perfect on the first try. That is why I have included the test and iterate step together. Once we have our prototype, we must bring it to the real world get feedback from real people. Return to the end user. Try to understand what is happening from their perspective. We can have patient’s fill out new intake forms, relocate the cleaning supply closet, and streamline the EHR. Then we gather the data and see where we can refine the idea. Did the solution work for them? Did it lead to a new problem? What additional insight have we gained?
After testing, it will be important to iterate on the solution. This might require us to circle back to the ideation or prototyping stages. At the heart of human-centered design is the notion that not every experiment or prototype will work. Design thinkers accept failure as part of the learning process. We shouldn’t be afraid of it. As Richard Branson, founder of the Virgin empire once said,
“Do not be embarrassed by your failures, learn from them and start again.”
Implement
Like I have mentioned before, no idea has any worth unless it is executed in real life. This requires having stakeholder buy-in that the solution is effective and worth pursuing. And then it is time to get to work. In my opinion, it is the least glamorous part of the design thinking methodology, but it is the most important. It might require retraining staff, rewriting protocols, and convincing naysayers in the hospital administration that the idea can work. As the idea becomes reality, there might still be moments to iterate and improve the unforeseen kinks, but implementation requires commitment, especially after the investments have been made. Implementation is all about hard work.
Like any process, design thinking isn’t perfect. Steve Vassalo, a product designer and investor, makes a point in his book, The Way of Design, that there is a risk that the term “empathy” no longer has any meaning. Instead it is just a Silicon Valley euphemism for market research, rather than the deeper ethnographic and anthropologic endeavor that was originally intended. Steve Jobs also pointed out that
“It’s really hard to design products by focus groups. A lot of times people don’t know what they want until you show it to them.”
So maintain balance by doing your research, building your prototype, and testing it and gathering feedback in real time. Don’t just follow the latest trends because people’s opinions often change.
Design thinking is searching for a solution as if it’s a moving target. It requires creative confidence, or the belief that it is okay to pursue a solution even if all the details haven’t been worked out yet. It requires trusting the process, embracing ambiguity, and giving yourself the permission to explore and fail. And it definitely requires a positive mindset to help keep the individual, the team, or the organization motivated and engaged. So what are you waiting for? We can all be designers now. It’s time to jump right in and start prototyping.
References